It’s 10:42 on a busy weekday morning when the red phone rings in the Emergency Department. You’re the junior doctor covering Resus. The nurse in charge looks up and says, “Ambulance incoming. Twenty‑four‑year‑old female. Sudden breathing difficulty. Suspected anaphylaxis.” You feel your pulse quicken. You’ve revised the algorithm countless times, but this is the first time you’ll be the doctor standing at the foot of the bed.
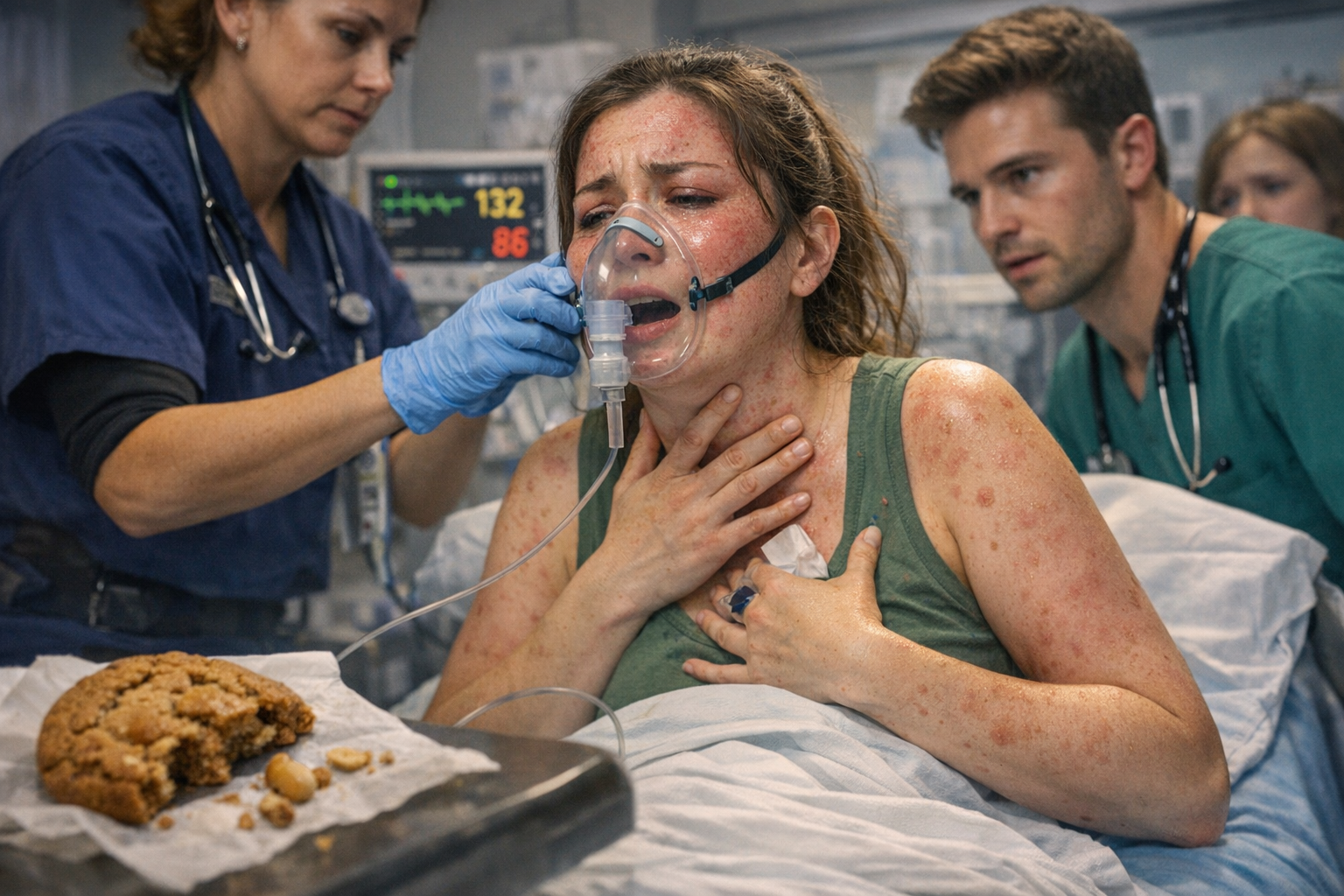
The paramedics wheel her in. She’s pale, clammy, and clawing at her throat. Her voice is barely audible as she forces out, “I… can’t… breathe…” You notice the widespread rash across her chest, the swelling around her lips and eyelids, the harsh wheeze with every breath. Her respiratory rate is racing, her oxygen saturations are low despite high‑flow oxygen, and her pulse is thready and fast. Her friend, breathless from running behind the trolley, blurts out that she ate a peanut cookie by accident and is severely allergic.
You know instantly that this is anaphylactic shock. There is no time to hesitate. You call for intramuscular adrenaline and focus on her airway, trying to position her so she can breathe while listening for signs of worsening obstruction. Her wheeze tightens, her voice disappears entirely, and for a moment you feel the room narrow to just her face and the sound of her breathing.
The nurse administers the adrenaline while another colleague secures IV access and starts fluids. Nebulised bronchodilators are prepared. Senior support arrives, but you are still leading the first critical minutes. When her blood pressure remains dangerously low, you repeat the adrenaline dose. Slowly, almost imperceptibly at first, her breathing begins to ease. Her colour improves. She manages a few words. The crisis begins to settle.
She is stabilised and transferred to the High Dependency Unit for observation. Her friend is crying with relief. Only now do you notice your own hands shaking – the adrenaline comedown after the adrenaline administration. The consultant turns to you and says, “Good call. Clear, decisive, safe. That’s what saves lives.” You realise the entire episode lasted less than twenty minutes, but it will stay with you for years.

I would stay calm by controlling my breathing, relying on my training, and following a clear, structured approach. Breaking the situation into simple steps would help me think clearly and act effectively under pressure.
Follow the steps that I’ve learnt making sure to breath steadily to stay focused so I can concentrate on the patient.